In-the-Ear Monitors & Hearing Conservation

Since the introduction of in-the-ear monitors (IEMs), engineers and performers have found them to be effective and flexible tools. They allow the engineer to customize each musician's monitor mix and clean up sound coming off the stage by partial or total removal of the conventional floor wedge monitors. The result is a reduction of the overall intensity levels on stage, feedback, and potential overexposure to loud sound. The flipside of IEM use is that if they are used improperly, IEMs can cause hearing problems. Some of these units are capable of delivering sounds at or near 130 dB SPL inside the ear canal.1 Regular misuse of IEMs may result in temporary or permanent damage to the sensory cells of the auditory system. Making physical modifications that alter the coupling or wearing IEMs at high intensities for long durations of time can increase the risk of problems.
When used properly, IEM systems have the potential to provide enormous benefit to the audio engineer and the performer. In addition to increased mobility and the improved isolation from amplifiers and crowd noise, IEMs can prevent vocalists from oversinging, which may result in permanent damage to the vocal cords and supporting musculature.2 The acoustic isolation they provide lets musicians monitor at lower intensities without sacrificing fidelity. This reduces the risk of overplaying and possible development of disorders associated with physical strain, such as tendonitits.3
Signal Flow: The Human Ear
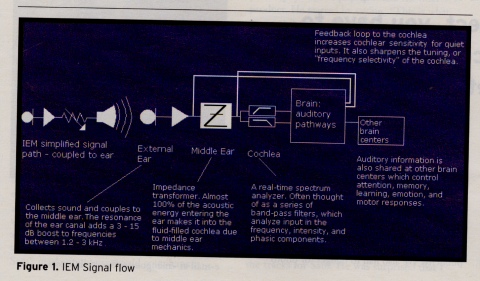
The auditory system is typically described in terms of its anatomy (the parts) and its physiology (what the parts do). However, the hearing mechanism can easily be described in terms more familiar to the audio engineer. Figure 1 [see below] is a diagram of the (simplified) signal flow of a generic IEM system, coupled to the human ear.

Effects of Overexposure
Before proceeding with the discussion of the benefits and risks of IEMs, it is important to discuss hearing loss in general. There are essentially three types of hearing loss a person could inherit or be susceptible to during his or her lifetime. They are conductive losses, sensorineural losses, and central auditory processing disorder (CAPD).
A conductive loss results from damage in the ear before the cochlea. Such losses may be caused by objects in the ear canal (such as excessive earwax or a cyst), a perforation or plaque growth onto or around the eardrum, growth onto or disarticulation of the middle ear bones, etc. Typically, a conductive loss can be successfully treated with either pharmaceutical or surgical remedies.
Sensorineural loss results from damage to the cochlea (the hearing organ) and/or ascending auditory nerve (the neural pathway leading to the hearing centers of the brain). A sensorineural loss is permanent, often progressive (becoming worse over time), and because it is neural damage, it cannot be fixed by medical or surgical intervention.
CAPD, sometimes called a "central loss," refers to damage or faulty processing in the hearing centers of the brain rather than a decrease in a person's ability to hear.
Damage from overexposure to loud sound results in a type of sensorineural loss often referred to as noise induced hearing loss (NIHL). Since NIHL evolved from clinical evaluations of noise exposure in industry and the military, the term isn't sensitive to the fact that every loud sound is not necessarily "noise," so in this article the term NIHL will not be used. It is important to be aware of the nomenclature when researching the subject.
Sensorineural hearing losses caused by overexposure to loud sounds can affect several parts of the body, and the hearing mechanism (cochlea) in particular. It is identified by a high-frequency loss with a characteristic steep-sloping drop in hearing sensitivity at or near 4 kHz .4 Although this probably occurs for many reasons, hearing loss due to general physiologic wear and tear in the cochlea is exacerbated by regular overexposure to loud sounds. Once damaged, the sensory (hair) cells responsible for the bioelectric transduction of sound lose their ability to function efficiently. With repeated exposure to loud sounds over time, the cell dies and eventually the adjacent hair cells and supporting cells become vulnerable.
This is why we experience hearing loss in broad-frequency regions, as opposed to one or two frequencies; our sensory cells don't die in isolation. Cell death affects adjacent cells, resulting in functional deficits across frequencies. If a sound is loud enough, even a "quick" sound (e.g., a burst of feedback or an extremely loud pop with the ear in close proximity to a speaker) can result in irreversible hearing loss. When a sudden loud sound causes an abrupt interruption of blood flow to the cochlea, resulting (behaviorally) in elevated hearing thresholds,5 it is clinically referred to as "acoustic trauma." It has also been noted that hearing loss from overexposure to loud sounds can also result in nonauditory problems.6 Examples include, but are not limited to, illness, headache, fatigue, insomnia, irritability, neuroticism, hypotension, hypertension, cardiac disease, colitis, endocrine disorders, biochemical disorders, and ulcers.
Benefits and Risks of IEMS
As stated previously, IEMs offer many benefits from the audio engineer's point of view. The overall fidelity due to the proximity of the amplifier to the eardrum is a significant improvement over wedge monitor systems. An experienced engineer can achieve sound quality with IEM systems that rival pro-studio headphones in dynamic range, breadth of frequency response, and clarity. The performer has increased mobility on stage, highly individualized mixes with individual volume controls on his or her beltpack, and acoustic isolation from amplifiers or other (non-IEM users) floor wedges.
Of course, the acoustic isolation (typically mentioned when discussing the benefits of IEM systems) can also be a problem.7 Most commercially available units don't allow easy communication between performers, as there is no microphone on the unit. Another drawback is that the earpiece needs to be taken out in order for the user to talk onstage, then it must be re-inserted. Noncustom earpieces (typically made of flanged silicone or foam) need time to expand after re-insertion. Many IEM users feel the acoustic isolation also produces a feeling of isolation from the audience. Blending an ambient mic into each performer's mix can help to reconnect the performer with the audience.
Performers should fully understand the appropriate use of IEMs. Due to the varying gain stages any band's setup may involve, the output of the IEMs may or may not be easy to measure. Although an audio engineer may try to keep the intensity levels low, an individual's control over the beltpack or a simple miscalculation of the gain stages could result in overexposure right at the eardrum. Since the earpieces are designed to achieve a tight acoustic seal, caution must be taken to avoid this problem.
When using a custom-molded IEM system, it is advisable to use either an internal or outboard peak limiter to provide some protection from transients and other sudden loud sounds that may occur during a performance.8 Custom-molded IEM devices are preferable because the acoustic seal and physical comfort they provide is superior. The efficient coupling of the amplifier and eardrum reduces the need to overamplify the mix for each musician. It is preferable to have the custom ear mold fitted by an audiologist, an expert in the clinical care of the ear. In turn, audiologists should guarantee an appropriate fit for your IEMs and should attend a rehearsal and/or a sound check to take probe microphone measurements. By placing a small microphone in the ear canal, an audiologist can measure how loud the performer's IEM is. The audiologist should then be able to recommend a preferred range of loudness for performances, thereby minimizing the risk of hearing loss.
Hearing Conservation Tips
Music and audio professionals should have their hearing professionally tested yearly. Ideally, audiologic services should include pure tone thresholds (including high-frequency audiometry), speech testing, acoustic immittance (tests middle ear function), and otoacoustic emissions.9High frequency audiometry will be the most difficult service to find because audiologists typically only test up to 8 kHz. It is important to know that the hearing health industry refers to 4-8 kHz as "high frequency." They reference their frequency range to speech frequencies, whereas an audio engineer typically refers to 12–18 kHz as high frequency. Musical sounds have a much broader bandwidth than speech. Although there are no established "normal" critera for high-frequency audiometry, test results may be compared over time, and these tests will be of benefit to music or audio professionals in the long run.
Typically sensorineural hearing loss from exposure to loud sounds is slow and progressive, and affects the high frequencies. By monitoring your high-frequency hearing, you will be able to see changes above 12 kHz, long before a loss shows up in the 4-8 kHz range that is of greatest concern to audiologists. Problems with understanding speech in noise, or (for a trained ear) noticing subtle timbre differences may be correlated with the loss of high-frequency acoustical information.10 If you feel you may be struggling to understand conversation in a noisy environment, but your pure tone audiogram reflects hearing within normal limits up to 8 kHz, serial testing of the higher frequencies may validate your complaint if thresholds consistently drop over time.
Part of the Job
Since exposure to sound is part of the job for the music or audio professional, it is important to take preventative steps rather than attempt to eradicate loud sound in an effort to conserve our hearing. There are several simple ways to conserve one's hearing.
Overexposure to loud sounds is defined by both the level of intensity and duration of exposure time. If one knows that a session or gig will be longer than usual, try to decrease the intensity level. Monitoring at louder levels may be acceptable, but only for short durations. Be aware of the locations of the P.A. system, amplifiers, and other sound sources. Standing directly in the critical path of the sound source will result in greater levels of exposure than standing at an angle from the source.11 After exposure, give your ears a rest. If total silence is not possible, go to a reasonably quiet place. If your session runs long, take frequent breaks. Without preventative measures like these, it will be easier to acquire a temporary threshold shift (TTS), and with repeated TTS, one acquires a permanent threshold shift (i.e., hearing loss).
In conclusion, IEMs, when used correctly, may offer a range of benefits for the performing musician and audio engineer. These include ease of transport, increased customization of mixes, improved sound quality, lowered stage volumes, and decreased overexposure to loud sounds for both the performer and the audience. Appropriate use of IEMs may also serve to protect your most valuable and irreplaceable instrument--your ears.
[ Also see the References page for this article ]
RACHEL CRUZ '93 holds a master's degree in audiology and hearing sciences from Northwestern University in Evanston, Illinois, and is a guest lecturer and author. She has also worked as an audio consultant and an audio engineer. Cruz is currently completing a clinical fellowship at the House Ear Institute in Los Angeles. She can be reached via e-mail at <rcruz@hei.org> or <cruzmediagroup@mindspring.com>.
In-the-Ear Monitors
REFERENCES
1. Hall, J., Santucci, M. (1995). "Protecting the Professional Ear: Conservation Strategies and Devices." The Hearing Journal, 48 (3).
2. Hart, C., Geltman, C., Santucci, M., Schupback, J. (1987). "The Musician and Occupational Sound Hazards." Medical Problems of Performing Artists, 2, 22-25.
3. ibid.
4. Katz, J. (ed.) (1994). Handbook of Clinical Audiology (fourth ed.). Baltimore: Williams & Wilkins.
5. Johnson, D., Krueger, R., Marentette, L. (1995). "Rock Concert Noise-Induced Hearing Loss." The Hearing Review, 2(5), 10-11. [See also Katz.]
6. Mueller, H.G.I., Hall, J.W. III (1998). Audiologists' Desk Reference, Volume II. San Diego, CA: Singular Publishers.
7. Trubitt, D.R. "Live Sounds: The Grateful Dead and Sting Do Vegas." Mix Magazine, September 1993.
8. Santucci, M. (1996). "Personal Monitors: What You Should Know." Mix Magazine, May 1996.
9. Santucci, M. "Protecting the Professional Ear: Conservation Strategies and Devices." The Hearing Journal, 48 (3), pp. 10-12.
10. Moore, B.C.J. (1997). An Introduction to the Psychology of Hearing (fourth ed.). San Diego: Academic Press.
11. Kryter, K. D. (1994). The Handbook of Hearing and the Effects of Noise: Physiology, Psychology, and Public Health. San Diego, CA: Academic Press.



